OUTPATIENT TREATMENT OF UMBILICAL HERNIA AND LINEA ALBA HERNIA
in Medical news
Posted on 03/14/2023
Outpatient treatment of umbilical hernia and linea alba hernia
By Doctor Patrick JULIENNE at the Clinique de Turin, Paris 8th arrondissement
Umbilical and white line hernias account for 25% of the 150,000 abdominal wall hernias operated on each year in France. The refinement of surgical techniques means that most operations can be carried out on an outpatient basis in complete safety. The cost savings to society are considerable, and the risk of nosocomial infection is reduced by this type of treatment.
Characteristics of umbilical and linea alba hernias
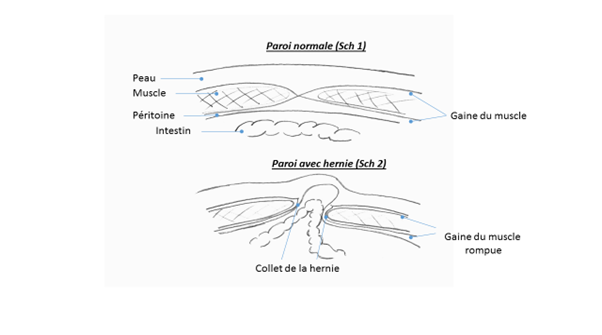
These hernias result from a rupture of the aponeurosis (or muscle sheath) at the level of the umbilicus, or on the so-called white line joining the umbilicus to the xiphoid process. They take the form of a permanent protuberance or a protuberance that becomes visible when coughing or exerting oneself. The neck of the hernia, which is the gap between the edges of the ruptured aponeurosis (see Diagram 2), connects the abdominal cavity containing the intestines with the hernia sac located under the skin.
They may be painless or a source of painful discomfort. Large hernias can strangle, requiring emergency surgery in poor conditions. The hernia is painful and can no longer be reintegrated into the abdomen. It may contain fat or even intestine, leading to occlusion. Large hernias can also cause skin irritation through rubbing. Umbilical and linea alba hernias must therefore be operated on cold before any complications arise. In the vast majority of cases, the operation can be performed on an outpatient basis.
They must be distinguished from :
- Diastasis of the rectus abdominis muscles, which sometimes causes a very large bulge between the umbilicus and the xiphoid process when the patient tries to stand up. Paradoxically, there is no risk and few surgical indications because the musculoaponeurotic wall is not ruptured.
- Eventration on the incision of a surgical operation where the musculoaponeurotic sheath has reopened in the following years. They require repeat surgery. Their incidence is currently increasing due to the frequency of laparoscopic surgery, where a trocar is inserted through an umbilical incision.
Laparotomy surgical techniques
In the vast majority of cases, apart from emergencies involving strangulation, this is a parietal operation without opening the abdominal cavity, and is performed on an outpatient basis. The technique involves
- Reintegration of the unopened peritoneal sac and its contents into the abdominal cavity.
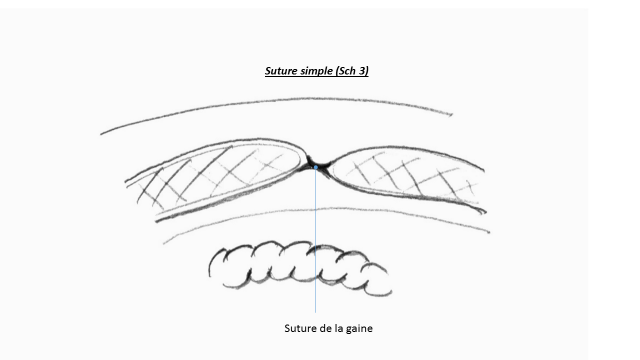
- Repair of the fascial breach by closing the neck:
~ Either by a simple suture if the neck is less than 12mm (see Diagram 3).
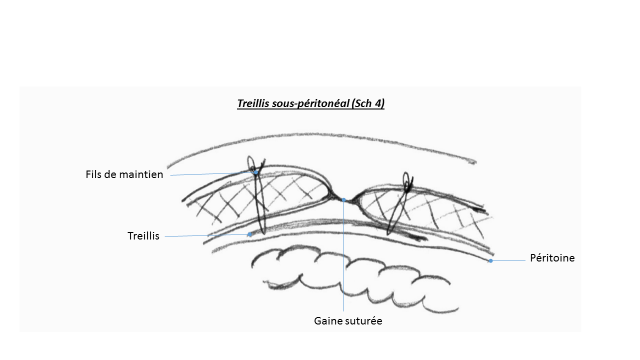
~ Or by a suture of the neck, but after detachment of the plane between the peritoneum and the muscle sheath for 3 cm all around the neck. A non-absorbable mesh is placed in this space, fixed by holding sutures passed through the muscle (see Diagram 4). The indication for reinforcing the sheath suture with mesh is multifactorial. A hernia neck of more than 12mm, future pregnancies, a patient who is obese or has a high level of physical, sporting or professional activity, or who is subject to coughing, are all factors which will influence the decision.
~ Rarely, apart from emergencies when an intra-abdominal procedure may be necessary, it will be necessary to open the peritoneum and place the parietal reinforcement plate in the abdominal cavity. (Diagram 5).
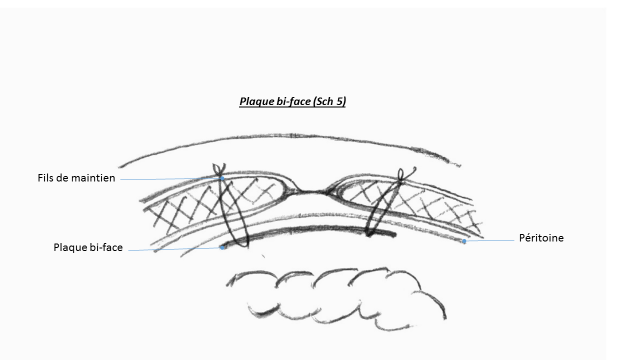
So-called two-sided plates are used, with one side gripping upwards into the muscular wall and a completely smooth side facing downwards, which will not adhere to the intestinal loops. The patient will then remain in hospital for 48 hours until transit resumes.
- In an emergency, in the event of strangulation, this surgical repair programme with a plate cannot always be carried out, particularly if resection of a portion of the intestine proves necessary. In the latter case, the use of a prosthesis is even contraindicated due to the risk of infection.
- Rarely, the condition of the skin may require resection of the umbilicus (omphalectomy).
- What is the role of laparoscopy? Laparoscopy requires the plates to be placed in the cavity of the abdomen, i.e. two-sided plates. In the case of walls that have not been operated on, as is the case with umbilical or linea alba hernias, the space between the peritoneum and the sheath is almost always free, allowing the mesh to be positioned safely without incursion into the abdominal cavity. On the other hand, laparoscopy seems to have its place in the treatment of ventrations, where the abdominal cavity would have to be opened by laparotomy in order to position the two-sided plate.
- Possible post-operative complications. Apart from those associated with any general anaesthetic, there may be bruising or even a serous effusion or haematoma in the former hernia pocket. These local complications usually resolve spontaneously. Infection, which is very rare, requires rigorous asepsis during the operation.
Finally, recurrence is also rare and will require a repeat operation.
Pre- and post-operative prescriptions for outpatient surgery
1. pre-operative
Surgical consultation
The surgeon informs the patient of the diagnosis, possible surgical techniques and the risk/benefit assessment of the operation. The patient is given written informed consent. Pre-operative hygiene rules are explained: An antiseptic shower the day before and the morning of the operation. Shaving or hair removal before the antiseptic shower in the morning. Prescription of painkillers and anti-inflammatories for the post-operative period, purchased before the operation. Since 2009, an estimate has been compulsory, indicating the fees that will be charged.
Anaesthetic consultation
In collaboration with the surgeon, patients eligible for outpatient surgery are selected on the basis of their general condition (ASA I or II as a rule), current treatment and whether they understand the postoperative prescriptions and can apply them at home. Pre-operative fasting rules specified and possible adaptation of the patient's medical treatments.
2. Post-operative
The patient is discharged at the end of the afternoon after a visit from the surgeon and anaesthetist. The patient must have passed urine. They may dress and walk before leaving the hospital. They will be accompanied until the next day by a trusted adult. Otherwise, they will remain in hospital until the following day. They must be able to contact their surgeon by telephone. Painkillers for the first 2 to 4 days. Sometimes an abdominal support belt must be worn for the first month after the operation. It is not necessary to make a follow-up visit for the first dressing the day after the operation if the monitoring procedures have been clearly explained and understood by the patient. An absorbable suture is usually placed on the skin, which does not require any sutures to be removed. One to four weeks' leave from work is prescribed, depending on the profession; on average, two weeks. A one-month break from sport or major physical activities, but walking is encouraged in the days following the operation. A check-up at 1 month before resuming all sporting activities.
Doctor Patrick JULIENNE










