OUTPATIENT INGUINAL HERNIA REPAIR
in Medical news
Posted on 03/13/2023
150,000 inguinal hernias operated on every year in France. This figure gives an idea of the scale of the public health problem. Over the last 25 years, surgical techniques have been refined, reducing the need for hospitalisation from 5-6 days to a cure that can usually be performed safely on an outpatient basis. The cost savings for society are considerable, and the risk of nosocomial infection is reduced by this type of treatment.
Outpatient treatment of Inguinal Hernia
By Doctor Patrick JULIENNE at the Clinique de Turin Paris 8th arrondissement
CHARACTERISTICS OF INGUINAL HERNIA
Inguinal hernias are the result of weakness in the abdominal wall and take the form of a protrusion in the groin, which may be permanent or protrude when coughing or exerting oneself. They may be painless or a source of painful discomfort. Large hernias can become strangulated (painful hernias most often containing intestine and leading to occlusion because they cannot be reintegrated into the abdomen), requiring emergency surgery in poor conditions. Inguinal hernias must therefore be operated on cold before complications arise. The Lichtenstein technique, which is currently the most widely used surgical technique, can usually be performed on an outpatient basis, which is the subject of this article.
THE LICHTENSTEIN TECHNIQUE
Inguinal hernia repair using the Lichtenstein technique aims to repair the weakened wall without putting any strain on the tissues. To achieve this, it uses a prosthetic reinforcement: a polyester mesh to reduce postoperative pain and the risk of recurrence.
Outline:
Under general anaesthetic or epidural The procedure begins with an injection of a local anaesthetic, Levobupivacaine, inside the anterosuperior iliac spine to block the sensory genital branches of the ilioinguinal and genitofemoral nerves. This block will help to sedate the pain for 6 to 8 hours after the operation. Incision 7 cm long in the suprapubic hair. Opening of the aponeurosis of the greater oblique muscle. In men, the hernia sac is isolated from the rest of the spermatic cord in the case of external oblique hernia and then resected or buried in the sub-peritoneal space. In the case of a direct hernia, it will also be buried by a concentric stitch placed at its base. In women, the hernia sac is usually resected.
Figure 1: EXTERNAL OBLIQUE HERNIA (spermatic cord below and hernia sac above)
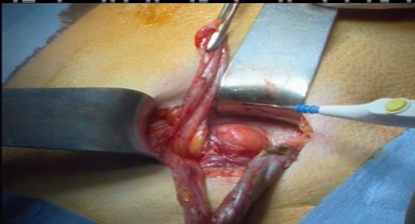
A prosthetic mesh (120 x 50 mm) is used to reinforce the deficient wall. In men, it is split down the middle to allow the spermatic cord to pass through. The mesh is secured with a few stitches, or even glued with the latest prostheses, and the aponeurosis of the oblique longus muscle is sutured in front of the mesh.
Figure 2: PROsthesis (white mesh) allowing passage of the spermatic cord
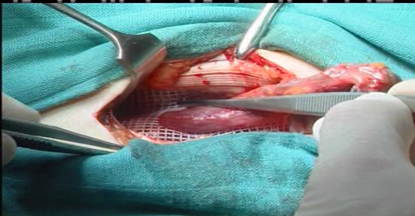
An absorbable intradermal suture completes the operation. There is therefore no thread to remove.
COMPARISON WITH OTHER INGUINAL HERNIA REPAIR TECHNIQUES
Schouldice:
This uses sutures from the patient's own tissues to repair the parietal weakness. In adults, the superiority of the Lichtenstein technique lies in the placement of the prosthetic mesh, which allows tension-free repair and reduces postoperative pain. The risk of long-term recurrence is reduced from 6% to less than 1%.
Laparoscopic mesh implantation:
Its advantage in comparative studies lies in a reduction in possible intermittent residual local discomfort. Only the surgeon, depending on the patient and the characteristics of the hernia, is in a position to propose one technique or another.
PRE- AND POST-OPERATIVE INSTRUCTIONS FOR OUTPATIENT LICHTENSTEIN SURGERY
Pre-operatively
Surgical consultation :
The surgeon informs the patient of the diagnosis, the possible surgical techniques and specifies the benefit/risk assessment of an operation. A written informed consent form is given to the patient. Pre-operative hygiene rules are explained: An antiseptic shower the day before and the morning of the operation. Shaving or hair removal before the antiseptic shower in the morning. Prescription of painkillers and anti-inflammatories for the post-operative period, purchased before the operation. Since 2009, an estimate has been compulsory, indicating the fees that will be charged.
Anaesthetic consultation
In collaboration with the surgeon, patients eligible for outpatient surgery are selected on the basis of their general condition (ASA I or II as a rule), current treatment and whether they understand the postoperative prescriptions and can apply them at home. Preoperative fasting rules are specified and the patient's medical treatment may be adapted.
Post-operative
The patient is discharged at the end of the afternoon after a visit from the surgeon and anaesthetist. The patient must have passed urine. They may dress and walk before leaving. They will be accompanied until the next day by a trusted adult. Otherwise, they will remain in hospital until the following day. They must be able to contact their surgeon by telephone. The only treatment consists of painkillers and anti-inflammatories for the first 2 to 4 days. There is no need for a follow-up visit for the first dressing the day after the operation if the monitoring procedures have been clearly explained and understood by the patient. One to four weeks' leave from work is prescribed, depending on the profession; on average, two weeks. A one-month break from sport or major physical activities, but walking is encouraged in the days following the operation. A check-up at 1 month before resuming all sporting activities.
Doctor Patrick JULIENNE










